

Ronish Gupta
McMaster University, Canada
Title: Rapid resolution of high-output chylothorax with reduction of spinal subluxation
Biography
Biography: Ronish Gupta
Abstract
Case Description:
A 2-year-old generally healthy boy with a history of limping gait presented and was admitted to a community hospital with severe Influenza A illness. There, he was intubated for refractory hypoxia, and found to have large bilateral pleural effusions. Bilateral chest tubes were inserted, draining > 1 L of milky fluid combined. He was transferred to the regional pediatric intensive care unit. With the effusions drained, he was easily extubated and biochemical testing confirmed the fluid to be chyle (triglyceride level = 3.48 mmol/L). Computed tomography scanning of the chest and abdomen was subsequently negative for malignancy, but incidentally found rib fractures, scapular fracture, and an unstable spinal subluxation (T11-L1). In the interim and during spinal surgical planning, the high-output chylothorax continued despite several days of NPO status with total parenteral nutrition (> 1L/d or > 50mL/kg/d). Following reduction and partial fixation of the spinal subluxation, the pleural drainage immediately ceased. Within 24-hours following surgery, the drainage became < 50mL/d. Two weeks later, the chylous drainage remained absent with the patient on a full enteral medium-chain triglyceride containing diet.
Discussion:
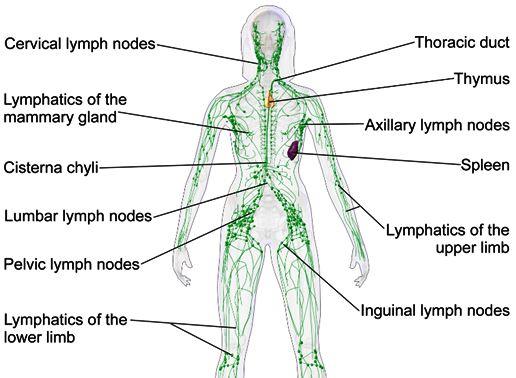
Acquired chylothorax in pediatrics is typically associated with mediastinal pathology (e.g. trauma, infiltrative), obstruction of drainage, or abnormal lymphatic vessel development. Case reports of chylothorax developing following spinal trauma and manipulation exist. This is, however, the first report to our knowledge of chylothorax resolution as a result of spinal intervention. Potential mechanisms include relief of obstruction of the cysterna chylii, the large lymphatic reservoir typically located adjacent to the L1-L2 vertebral bodies. Patients with chylothorax in the context of thoracolumbar spinal pathology may warrant consideration of an intervention aimed at relieving any potential lymphatic obstruction.
Recent Publications
1. Pillay TG, Singh B. A review of traumatic chylothorax. Injury. 2016;47(3):545-550. doi:10.1016/j.injury.2015.12.015.
2. Bender B, Murthy V, Chamberlain RS. The changing management of chylothorax in the modern era. Eur J Cardio-thoracic Surg. 2016;49(1):18-24. doi:10.1093/ejcts/ezv041.
3. Ichikawa Y, Sato A, Sato K, et al. Chylothorax associated with child abuse. Pediatr Int. 2015;57(6):1202-1204. doi:10.1111/ped.12707.
4. Mora de Sambricio A, Garrido Stratenwerth E. Chylothorax following anterior thoraco-lumbar spine exposure. A case report and review of literature. Rev Española Cirugía Ortopédica y Traumatol (English Ed. 2015;59(2):129-133. doi:10.1016/j.recote.2015.01.002.
5. Gartside R, Hebert JC. Chylothorax following fracture of the thoracolumbar spine. Injury. 1988;19(5):363-364.